2018 marks the 20th anniversary of Stichting HIV Monitoring’s ATHENA cohort. In the past two decades, the AIDS Therapy Evaluation in the Netherlands cohort, which started in 1998 as a three-year project, has undergone various developments with important consequences for all those involved, such as people living with HIV, HIV-treating physicians, HIV nurses and Stichting HIV Monitoring (SHM) staff. Here we look back over the past 20 years with people involved both at the start and today.
‘We used to collect everything on paper, noting down by hand all the information from the medical records, which we used to carry back and forth,’ remembers Yolanda Ruijs-Tiggelman. Yolanda began as a data collector for the project back in 1999 and is still employed by SHM today. Her colleague, Lia Veenenberg-Benschop, adds ‘It’s almost impossible now to think that we were sat in that tiny room in the AMC’. She too has worked for SHM for almost 20 years.
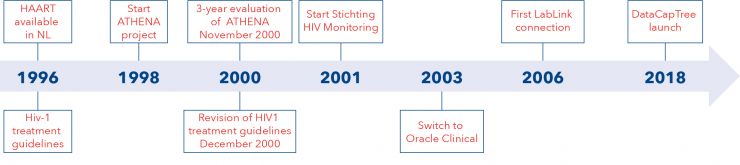
ATHENA was the result of a revolutionary development in HIV treatment. During the international AIDS conference in 1996 in Vancouver, the first results were presented on the use of triple therapy. ‘The approach was new because it combined a total of three drugs from two different classes, which was found to be sufficient to prevent selection of resistance and to maintain a suppressed viral load,’ says Peter Reiss, professor of internal medicine at Amsterdam UMC (AMC site) and director of SHM since 2013. ‘It was a real breakthrough and I saw its effect in the clinic: people who would have previously died, were surviving!.'
In the Netherlands, the minister of public health at the time, Els Borst, arranged for people living with HIV to have accelerated access to this new triple therapy. However, she also insisted that the impact of this novel approach be properly assessed. As a result, the ATHENA project was set up. One of the people who ensured that the project got off the ground was Frank de Wolf, professor at Imperial College London and past director of SHM. ‘We wanted to develop a system with which we could predict when to start the treatment and, to do so, needed to collect enough data. The second goal was to have a system for measuring whether people were actually responding well to the treatment.’ Frank de Wolf set up ATHENA together with the late Joep Lange, and the project was launched in the summer of 1998.
The community of people living with HIV played an important role in the whole process. ‘Those guys were young and, albeit infected with HIV, still healthy and able to accomplish a great deal. They were well organised and knew exactly what they wanted; this helped us enormously in moving forwards. It’s not something you see very often nowadays,’ remembers Frank de Wolf.
The significant improvement in the patients soon became apparent and people could start looking to the future again. However, it also became clear that keeping up this new treatment was a challenge. ‘People had to take large numbers of pills, several times a day,’ says Peter Reiss. ‘In addition, new side effects started to appear, such as an altered physical appearance due to loss of subcutaneous fat in the arms, legs and face and an increase in other areas (known as lipodystrophy), which brought further stigmatisation with it. This meant it was even more important to find out why this was happening’. Although the initial culprit was thought to be the new drugs, it turned out later to actually be due to older drugs such as d4T and AZT.
In the first three years, the ATHENA project confirmed that the new triple therapy was life-saving. However, it also became clear that longer-term monitoring was necessary for issues such as resistance and side effects. This required a more permanent structure to allow continued data collection. As a result, Stichting HIV Monitoring was set up to manage the cohort, a move that has proven its value many times over.
‘We had already been seeing side effects in daily practise,’ says Nienke Langebeek, HIV nursing specialise at Rijnstate hospital, ‘and these were confirmed by the collection of data, from the ATHENA cohort, which was an excellent source of information. Furthermore, as people with HIV started living far longer than before the cART era, we started seeing different things in clinical practice that could be verified by SHM and the ATHENA cohort.’
Ard van Sighem, senior researcher at SHM remembers another example of the value of the ATHENA cohort: ‘Around 2005 we did some research for the Association of Insurers to investigate whether, with the advent of the new therapies, life insurance could be affordable for people living with HIV. Our data provided confirmation that this was the case. This was a really tangible effect, with significant impact for society, and only possible because of the existence of SHM and the ATHENA cohort.’
The success of triple therapy meant people stayed alive, became older and consequently started to suffer more from age-related illnesses, such as cardiovascular disease. However, it was unclear to what extent these illnesses were exacerbated by the HIV drugs. One of the initiatives set up to look into this issue was the successful international D:A:D study (Data collection on Adverse effects of anti-HIV Drugs), to which ATHENA, through SHM, made an important contribution. The information generated by the D:A:D study has influenced treatment guidelines on various occasions.
One of the people involved since the early days of the ATHENA project is Sima Zaheri, now deputy director of SHM. At the start of ATHENA she worked as a data monitor, later becoming responsible for setting up the data quality unit and processes for SHM. ‘ATHENA was born from the need to optimise care for people living with HIV,’ explains Sima Zaheri. ‘Everyone sensed the urgency and it was vital that the data were of good quality and reliable. After all, these data are used for research that is directly related to care. People were very motivated and the sense of involvement was palpable.’
One of the first large projects facing SHM was the creation of a centralised database, by switching to a data entry system based on an Oracle Clinical data management system. Together with the clinical research unit of the AMC hospital, a module was built in Oracle Clinical for SHM’s data collection process. Prior to this, the collected data were stored locally at each treatment centre. ‘This could negatively affect data quality,’ explains Sima Zaheri. ‘For example, if a code was added for a new drug, it was put on a CD-ROM and someone had to drive across the country installing it on all the computers. And of course, sometimes things went wrong and a hospital might end up working with an out of date version of the data collection protocol.’
Yolanda Ruijs also experienced the benefits of centralisation. ‘You can hardly imagine it now, but in the past I drove all over the country to collect the clinical report forms so that they could be entered into the database at our head office. Everything was coded of course, but still…’. As a result of the digitalisation move, it became possible to put an end to hand-noting all the data on site and instead the data that were previously stored locally could be collected in a central location.
Right from the start, ATHENA, and later SHM, has been involved in international collaborations between cohorts. Ferdinand Wit, HIV-treating physician at Amsterdam UMC (AMC site) and senior researcher at SHM says: ‘We have always taken part in these collaborations. By pooling the data from several cohorts we can answer questions that no single cohort alone has the power to answer.’ One of the reasons that the data from the ATHENA cohort are so valuable is the nationwide coverage within the cohort. ‘If you want to find out something about the HIV epidemic in the Netherlands or about certain facets of the epidemic, you don’t need to make an estimate or take random samples. Instead you can use data from almost all the people in care. It’s a real luxury,’ says Ferdinand Wit.
Both Frank de Wolf and Peter Reiss describe the situation in the Netherlands as unique. ‘Internationally, it was an enviable situation. Everyone thought it was an exceptionally good idea and that it had been well set up,’ says Frank de Wolf. In addition to contributing to the previously-mentioned D:A:D study, ATHENA data have also contributed to other international collaborations such as EuroCoord. ‘Due to the nationwide coverage, we have always played an important role in international collaborations, as well as in scientific publications. We are also an important partner when discussing intrinsic issues within these collaborations,’ adds Peter Reiss.
This is confirmed by Bruno Ledergerber, HIV researcher at the University of Zurich, who has been closely involved in many of the European collaborations in which ATHENA participates: ‘The ATHENA cohort is renowned for its high-quality and highly representative data that are collected by Stichting HIV Monitoring, and has made valuable contributions to international collaborations such as D:A:D, ART-CC, COHERE and EuroCoord’.
Investment in data quality has always been a priority. Not just in terms of technology and digitalisation, but also in terms of training. For example, new data collectors follow a tailored training programme and all data collectors attend regular review days. SHM’s data collectors have also played an important role in the most recent technological development, namely the new data entry system, DataCapTree, that was launched earlier this year. ‘Thanks to the strong collaboration between the research group, the construction group and the data collectors, we have produced a fantastic product. Moreover, we now have an in-house team that is not only familiar with the content, but also understands the technical aspects of the system,’ says Sima Zaheri.
In a year’s time it will be possible to measure the effects of DataCapTree on both efficiency and quality, and there are still many other IT-related plans for the future, according to Sima Zaheri: ‘If hospitals were to use certain standards for noting information in the electronic patient records, we could use such standards to collect all the data from the patient records in one go, for example, just as we now do for laboratory data using LabLink.’ Such developments would allow data collectors to collect the required information more quickly. Sima Zaheri also believes that it would be worth exploring the possibility of linking with other relevant quality registrations, providing due care is given to the challenges posed by the privacy legislation.
The implementation of PrEP in 2019 will also throw up new challenges for the data collection protocols, for example the registration of previous PrEP use by a person newly-diagnosed with HIV. ‘It is important to keep adapting the data collection process to any new developments and needs from the field that may have implications for monitoring the epidemic,’ says Peter Reiss.
In the future, the ATHENA cohort will continue to play an important role in monitoring the course of the HIV epidemic, according to Birgit van Benthem of the Centre for Infectious Disease Control of the National Institute for Public Health and the Environment (RIVM-CIb). SHM’s data are used for policy development and national and international reporting by the RIVM. ‘The ATHENA cohort is, and will remain, an important source of information with which to evaluate whether certain goals have been achieved, such as those formulated in the national plan for action on STIs, HIV and sexual health,’ says Birgit van Benthem. This is backed up by the director of the HIV association, Pieter Brokx, who says: ‘The detailed data collection provides good insight into the epidemic and makes it possible to monitor the quality of care and treatment and make adjustments where necessary’.